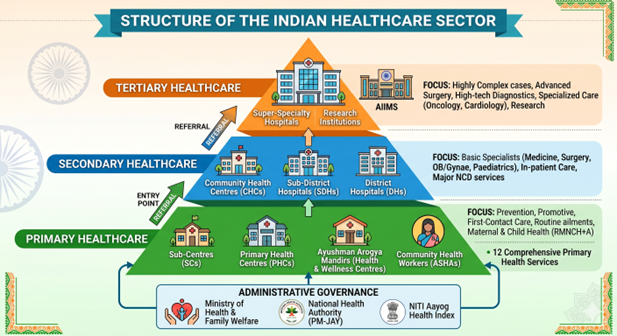
In India, the healthcare system is structured hierarchically into three distinct levels: Primary, Secondary, and Tertiary.
Primary Health Sector: The Foundation
-
- Role: The first point of contact between the individual and the healthcare system. It deals with 80-90% of healthcare needs through prevention, promotion, and routine curative care.
- Key Interventions: Maternal and Child Health (RMNCH+A), immunization, basic nutrition, screening for Non-Communicable Diseases (NCDs).
- Evolution: Under Ayushman Bharat, traditional Sub-Centres and PHCs are upgraded to Ayushman Arogya Mandirs (Health & Wellness Centres) to provide a comprehensive package of 12 services, expanding beyond basic maternal care.
- Workforce: Primarily staffed by Mid-Level Health Providers (MLHPs/CHOs), Auxiliary Nurse Midwives (ANMs), and supported externally by ASHA workers (community facilitators).
Secondary Health Sector: The Bridge
-
- Role: Provides care requiring more specialized knowledge or equipment, usually on referral from the primary level.
- Facilities: Community Health Centres (CHCs): 30-bed hospitals serving a block.
- Sub-District Hospitals (SDHs) & District Hospitals (DHs): Providing advanced secondary care.
- Specialties: Mandated to have basic specialists—Medicine, Surgery, Obstetrics & Gynecology, and Pediatrics—along with basic X-ray and laboratory support.
- Status: This is often the weakest link in India, facing chronic shortages of specialists, leading to overcrowding at the tertiary level.
Tertiary Health Sector: The Specialized Peak
-
- Role: Focused on the most complex medical conditions requiring highly specialized staff and advanced technology.
- Facilities: Medical Colleges and Hospital Complexes (like AIIMS or Post Graduate Institutes), and apex single-specialty institutions (e.g., Regional Cancer Centres).
- Focus: Advanced surgeries (neurosurgery, transplants), trauma care, intensive care, high-tech diagnostics, and medical education/research.
- Funding: Receives disproportionately high funding compared to the primary sector, a major point of policy analysis.
| Feature | Primary Level | Secondary Level | Tertiary Level |
|---|---|---|---|
| Focus | Prevention & Primary Care | Specialized Curative Care | Super-Specialty & Complex Care |
| Staff | MLHPs, ANMs, ASHAs | General Specialists (e.g., Surgery) | Super-Specialists (e.g., Cardiology) |
| Complexity | Low | Medium | High |
| Funding Burden | State-funded (with NHM help) | State-funded/District budget | Large Central/State outlays; PM-JAY |
| Coverage | Population-wide (Universal) | 80,000–1.2 Lakh (per CHC) | Regional/State population |
India faces an “inverted pyramid” in healthcare utilization. Due to weak primary and secondary care (lack of doctors, diagnostics), patients with minor ailments (fever, standard deliveries) directly bypass them to access major tertiary hospitals (like AIIMS), causing massive overcrowding and resource waste at the apex.
THE INFRASTRUCTURAL GAPS
Primary Tier: The Access Gap
The primary level (Sub-Centres and PHCs) is the foundation. While many have been upgraded to Ayushman Arogya Mandirs (AAMs), functional barriers persist.
-
- Electrification & Utilities: As of late 2025, approximately 24% of PHCs still face unreliable electricity or lack sustainable power sources. This renders high-tech equipment, vaccine refrigerators, and diagnostic tools useless.
- Building Status: Many centers continue to operate out of rented buildings or dilapidated structures that lack basic sanitation and running water, especially in hilly and tribal terrains.
- Bed Deficit: A significant number of PHCs (nearly 60% in certain high-priority states) lack the mandated 4–6 bedsfor basic observation or stabilize-and-refer cases.
- Diagnostic Lag: While the “Free Diagnostics Initiative” covers 14–63 tests, the “Hub and Spoke” model often fails due to poor sample transport logistics from remote villages to district labs.
Secondary Tier: The Specialist Gap
The secondary level (CHCs and District Hospitals) is often called the “Missing Middle” of Indian healthcare infrastructure.
-
- Specialist Shortage: This is the most critical infrastructure gap. Recent data (2025-26) shows a shortfall of nearly 5% to 80% of specialists (Surgeons, OB-GYNs, Physicians, and Pediatricians) at CHCs.
- Surgical Capacity: Many CHCs lack functional Operation Theatres (OTs) and Blood Storage Units. Without these, the facility cannot act as a “First Referral Unit” (FRU) for emergency C-sections or trauma.
- Equipment Maintenance: There is a high “CAPEX-OPEX” gap. While buildings are constructed, there is a lack of Operations & Maintenance (O&M) budgets, leading to broken X-ray machines and non-functional oxygen plants.
Tertiary Tier: The Overcrowding Gap
The tertiary level (AIIMS, Medical Colleges) suffers from “Referral Backflow”—treating cases that should have been handled at lower tiers.
-
- Bed-to-Patient Ratio: Despite new AIIMS being established, the bed density in tertiary public hospitals remains low (~0.5 per 1,000 population), leading to patients being treated on stretchers or floors in corridors.
- Critical Care Deficit: Before PM-ABHIM, only a handful of district hospitals had dedicated critical care blocks. The current transition is slow, with a persistent shortage of high-end ventilators and ICU staff.
- Diagnostic Quality: Only about 2% of laboratories in India (mostly private tertiary) have NABL accreditation. Public tertiary centers often face long backlogs (sometimes months) for advanced tests like MRIs or Biopsies.
| Tier | Primary (AAM) | Secondary (CHC/DH) | Tertiary (Medical Colleges) |
|---|---|---|---|
| Main Gap | Functionality (Power/Water) | Specialists (80% Shortage) | Overcrowding (Referral Gaps) |
| Tech Gap | Low Digital Literacy/Connectivity | Lack of O&M for Equipment | Data Silos (Non-interoperable) |
| Impact | High Out-of-Pocket Spend | Bypassing to Tertiary Care | High Mortality in Critical Cases |
The Pradhan Mantri Ayushman Bharat Health Infrastructure Mission (PM-ABHIM), with an outlay of ₹64,180 crore (2021–2026), is India’s most ambitious attempt to plug functional gaps across all healthcare tiers. Unlike previous schemes that focused on “building clinics,” PM-ABHIM is designed for “Pandemic Preparedness” and “Critical Care.”
Spread the Word