THE CONTEXT: Globally, close to 800 000 people die by suicide every year; that’s one person every 40 seconds. While the link between suicide and mental disorders (in particular, depression and alcohol use disorders) is well established, many suicides happen impulsively in moments of crisis. Suicide is an emerging and serious public health issue in India. We have witnessed spate of suicides reported among school students preparing for competitive exams in Rajasthan’s Kota. This article explains the causes and impacts of suicides in India and strategies to address them from the UPSC perspective.
INDIA’S STAGGERING CONTRIBUTION TO THE CRISIS
- In India, the situation is even more alarming. Data from the National Crime Records Bureau (NCRB) reveals that in a recent year, India recorded an average of 381 suicides daily, contributing to 17.8% of global suicides. This positions India as having one of the highest suicide rates in the south-eastern Asian region.
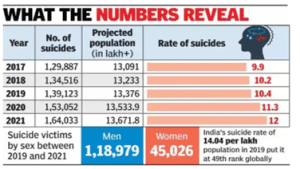
- The number of deaths due to suicides in India reached an all-time high in 2021, according to the latest data from the National Crime Records Bureau.
- In 2021, the rate of suicide – the number of death due to suicides per one lakh population – stood at 12. This is the highest rate of deaths from suicides since 1967, the earliest year for which data is available.
- The highest numbers of suicides were reported in Maharashtra where 22,207 persons killed themselves in 2021. This was followed by Tamil Nadu at 18,925 suicide cases, Madhya Pradesh at 14,965, West Bengal at 13,500 and Karnataka at 13,056.
- Beyond mere numbers, the patterns within these statistics – such as the predominance of youth, the rural-urban divide, and gender-specific trends – highlight the multi-dimensional challenges India faces. The intersection of socio-economic pressures, cultural nuances, and mental health stigma further exacerbates the crisis.
- National Data: India’s national average, as per the latest NCRB report, stands at about 11 suicides per 100,000 people. This figure is higher than the global average, emphasizing the gravity of the situation.
- State-wise Data: Disparities exist between states. For instance, southern states like Tamil Nadu and Kerala report higher suicide rates than the national average, while northern states like Punjab and Haryana report rates below the average. States with reported agrarian distress, like Maharashtra, show an uptick in farmer suicides.
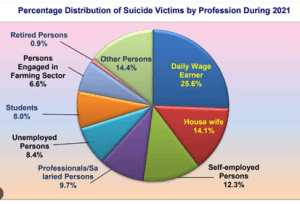
- The share of students among India’s overall suicide victims has also increased. It stood at 8% of the total in 2021, having grown by 2.3 percentage points since 2011.
As we delve deeper, we’ll analyze the intricacies of India’s suicide rates, hoping to shed light on the systemic and societal changes needed to mitigate this pressing concern.
HISTORICAL CONTEXT
EVOLUTION OF SOCIETAL VIEWS ON SUICIDE IN INDIA:
India’s views on suicide have undergone significant changes over millennia, mirroring its socio-cultural evolution.
Historically, during the Vedic period, there were instances where ‘self-sacrifice’ was not only accepted but celebrated under specific circumstances, like the practice of “Sati” where some widows were expected (or forced) to self-immolate on their husband’s funeral pyre. While the act itself was tragic, it was symbolically viewed as a profound display of loyalty and honor.
In later periods, especially during the time of the Dharmashastras, suicide began to be seen in a more negative light. Traditional texts often prescribed penalties in the afterlife for those who took their own lives, reinforcing the notion that suicide was a grave sin.
INFLUENCE OF CULTURAL, RELIGIOUS, AND TRADITIONAL BELIEFS:
- Hinduism: The ancient Hindu scriptures, the Vedas and the Upanishads, do not specifically discuss suicide, but later scriptures like the Puranas detail consequences in the afterlife for those who end their own lives. The Bhagavad Gita, while not directly referencing suicide, emphasizes the sanctity of life and the importance of performing one’s duty (dharma).
- Buddhism: Buddhism traditionally views life as a cycle of birth and rebirth, with suffering (dukkha) central to human existence. Taking one’s own life interrupts this cycle and is thus considered undesirable. Suicide, by creating more suffering, is seen as contradictory to the Buddhist path.
- Islam: With a significant Muslim population, India’s Islamic community views suicide as haram (forbidden). The Quran explicitly states that one should not kill oneself.
- Jainism: Jainism introduces a nuanced perspective with the practice of ‘Sallekhana’, where an individual voluntarily gives up food and water to embrace death. This is not considered suicide but rather a religious act of purifying the soul.
- Christianity: India’s Christian community views suicide through the lens of the Bible, which emphasizes the sanctity of life. While suicide is not explicitly mentioned, it’s generally perceived as a grave act against God’s gift of life.
Suicides, especially those connected with religious or cultural practices in India, have been a significant concern.
Santhara: A practice in the Jain community where an individual, typically at a very old age, chooses to embrace voluntary death by fasting. This came under scrutiny when the Rajasthan High Court in 2015 declared the practice as illegal, equating it to suicide. However, the Supreme Court, in a subsequent ruling, suspended the High Court’s decision.
The Supreme Court has emphasized the importance of the right to life under Article 21 of the Constitution. While historically, attempting suicide was a punishable offense under Section 309 of the Indian Penal Code, the Mental Healthcare Act, 2017, decriminalized it, recognizing that persons attempting suicide are in need of care and support.
Émile Durkheim
Émile Durkheim, a pioneering sociologist, identified four distinct categories of suicide in his seminal work, “Suicide” (1897): egoistic, altruistic, anomic, and fatalistic. Let’s discuss these categories within the Indian context:
- Egoistic Suicide: This results from an individual’s detachment from society. When societal bonds weaken, individuals face existential crises leading to such suicides. In India, urbanization and the erosion of traditional joint family systems can be seen as factors intensifying feelings of isolation, especially among the elderly, leading to increased vulnerability to egoistic suicide.
- Altruistic Suicide: Here, individuals are too integrated into societal norms, leading them to end their lives for a perceived greater good. Historically, the practice of ‘Sati’ (widow immolation) and ‘Jauhar’ (mass self-immolation by women to avoid capture) can be viewed through this lens. Although outlawed and largely eradicated, such practices reflect the deep cultural roots of altruistic suicide in parts of India.
- Anomic Suicide: Stemming from sudden disruptions in individuals’ lives, leading to an inability to cope. Economic downturns, job losses, or societal upheavals can lead to this. In the Indian context, the farmer suicides, especially in states like Maharashtra, can be attributed to anomic factors where economic hardships, unpredictable monsoons, and debt burdens precipitate tragic outcomes.
- Fatalistic Suicide: Although Durkheim didn’t extensively discuss this in his work, it implies suicide resulting from oppressive societal norms. In the Indian context, it can be linked to individuals who face insurmountable societal pressures, like LGBTQ+ individuals in traditionally conservative areas or young lovers from different castes or religions facing societal backlash.
Understanding Durkheim’s categories in the Indian context provides a lens to analyze the diverse sociocultural factors influencing suicide. With India’s intricate tapestry of tradition, rapid modernization, and societal norms, addressing the root causes necessitates a deep understanding of these categories and the regional and cultural nuances attached to them.
CONTEMPORARY PERSPECTIVE ON SUICIDE IN INDIA
Modern India stands at the crossroads of rapid socio-economic development, digital globalization, and deeply rooted traditional beliefs. This unique intersection has shaped the nation’s contemporary views on suicide:
- Media’s Role: With the proliferation of digital media, discussions around suicide are becoming more frequent. However, media coverage can be a double-edged sword. Sensationalized reporting can sometimes inadvertently lead to “copycat” suicides, prompting calls for more responsible and sensitive portrayals of the issue.
- Urban-Rural Divide: Rapid urbanization and the stress of city life have led to an increase in the number of suicides in metropolitan areas. On the other hand, agrarian distress, especially in states like Maharashtra and Telangana, has been a driving factor behind rural suicides.
- Mental Health Awareness: There’s a growing recognition of mental health issues as significant contributors to suicide. Initiatives like the Mental Healthcare Act 2017 reflect a shift towards decriminalizing suicide and emphasizing the importance of mental well-being. Despite this, stigmas persist, especially in rural and conservative pockets, making it challenging for many to seek help.
- Educational Pressures: The increasing importance placed on academic excellence and the competitive nature of entrance examinations have put immense pressure on the youth. Instances of student suicides post-exam results have instigated debates on the education system and its inherent pressures.
- LGBTQ+ Community: With the decriminalization of homosexuality in 2018 (Section 377), there’s been a renewed focus on the mental health challenges faced by the LGBTQ+ community. Despite legal progress, societal acceptance is still evolving, and many from the community grapple with issues of identity, discrimination, and mental health, sometimes leading to self-harm.
- Legislation and Intervention: While suicide was decriminalized in 2017, the act of attempting suicide was only recently decriminalized, marking a shift from punishment to rehabilitation and care. More helplines, NGOs, and counselingcenters are sprouting across urban centers, signaling a more proactive approach to the issue.
AN ANALYTICAL LOOK AT DEMOGRAPHIC VARIATIONS
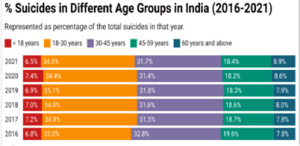
- Age: The age group of 15-29 years consistently reports a higher incidence of suicide. The pressures of academic performance, early career challenges, and personal relationships often collide during these formative years, increasing vulnerability.
- Gender: While more men commit suicide in absolute numbers, the rate of suicide attempts is reportedly higher among women. The disparity could be due to societal pressures, domestic issues, and the methods used.
- Urban vs. Rural: Rural areas, especially in regions facing agrarian crises, register a higher suicide rate. The stressors here, like indebtedness and crop failure, are starkly different from urban stressors, which often revolve around isolation, professional pressures, and lifestyle challenges.
FEMALE SUICIDES IN INDIA
- Irrespective of education and financial independence, women are still not as empowered as we would like to believe. Gender-based discrimination is still prevalent, and this inherent bias is reflected in the high number of female suicides.
- India’s female suicide burden is enormous. Indian women make up 36 percent of all global suicides in the 15 to 39 years age group – the highest share of any nation in the world.
- National Crime Records Bureau (NCRB) 2021 has thrown light on some grim trends, fuelling concern over mental health and social status of women in India.
- A total of 1,64,033 suicides were reported in the country during 2021, showing an increase of 7.2 percent in comparison to 2020. Housewives constitute a major chunk of these deaths.
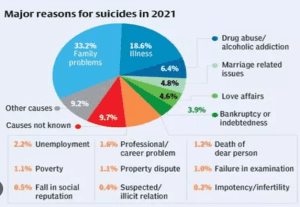
- Family problems, illnesses, and marital issues are the principal contributors behind female suicides in India.
- Family problems, illness, love affairs, and failure in exams emerged as the chief causes behind suicide deaths of girls below the age of 18 years in India.
- A seminal Lancet Public Health study (2018) on suicides in Indian women speculates that the increasing number of female suicides may be related to a conflict between women’s increasing education and empowerment and the persistence of their lower status in Indian society.
UNDERLYING CAUSES FOR SUICIDES IN INDIA
SOCIETAL PRESSURE
- Academic and Career Expectations: The hyper-competitive nature of India’s educational system, with a limited number of seats in prestigious institutions and an emphasis on certain lucrative professions, puts immense pressure on students. Failure to meet these expectations can lead to a sense of hopelessness and despair. It is also because of the ‘left behind syndrome’ among the students.
For instance, As many as 23 students have reportedly died by suicide in Kota this year; 15 took the extreme step in 2022.
- Marital and Family Issues: Familial and societal expectations surrounding marriage, including dowry demands and pressures to bear children (preferably male), can create significant distress. Additionally, marital discord, domestic violence, and forced unions contribute to the vulnerability of individuals, particularly women. The National Family Health Survey (2019-21) highlights the challenging circumstances faced by married women, including limited mobility, restricted financial autonomy, and marital control, as well as physical, sexual, and emotional abuse at the hands of their spouses.
For instance, The number of women who died by suicide in India reached a peak of 45,026 in 2021. More than half of them were housewives. The share of housewives in total female suicides is above the 50% mark.
MENTAL HEALTH
- Prevalence of Mental Health Disorders: Mental disorders, particularly depression, anxiety, and bipolar disorder, are significant contributors to suicides. Often, these conditions remain undiagnosed and untreated.
- Stigma Associated with Seeking Help: The societal stigma surrounding mental health often prevents individuals from seeking help. Many see mental health issues as a sign of weakness or a source of shame, rather than treatable conditions.
ECONOMIC FACTORS
- Financial Stress and Unemployment: Economic disparities and lack of stable employment opportunities, especially in densely populated urban areas, lead to financial instability and resultant stress, driving individuals to despair.
- Farmers’ Suicides and Their Causes: The agrarian sector has witnessed a surge in suicides. Factors include crop failure, rising debts, inability to repay loans, and climate-induced challenges. Lack of access to modern agricultural tools, techniques, and fair pricing further exacerbate their vulnerability.
ACCESS TO MEANS
- Pesticide Ingestion: As previously mentioned, the easy availability of toxic pesticides, particularly in rural settings, provides a lethal means. Restricting access to such substances could act as a preventative measure.
- Hanging: Being a method that requires minimal resources and provides little opportunity for rescue or reversal, hanging becomes a common choice.
- According to the NCRB data, in 2021, 57 per cent of the total suicides occurred by hanging, while 25.1 per cent happened by poison consumption.
CULTURAL AND SOCIAL ASPECTS
- Honour and Shame Dynamics: In many parts of India, family honor is paramount. Instances of perceived “dishonour,” like inter-caste relationships, can lead to extreme measures, both by the individuals involved and by family members.
- Role of Caste and Communal Issues: Caste-based discrimination and communal tensions have been sources of significant distress in the country. Marginalized individuals, especially from lower castes, often face systemic discrimination, leading to feelings of hopelessness.
For instance, Rohith Vemula, Darshan Solanki, Aniket Ambhore, Payal Tadvi. The common link between these alleged suicides is caste discrimination and harassment.
The interplay of multiple factors, from societal expectations and economic pressures to mental health challenges and access to lethal means, converge to make suicide a pressing issue in India. Addressing it requires multi-pronged, empathetic, and culturally sensitive approach.
THE RIPPLE EFFECT OF SUICIDE
IMPACT ON FAMILIES AND COMMUNITIES
- Grief and Trauma: The immediate family members experience profound grief, often accompanied by a sense of guilt, wondering if they could have done something to prevent the tragedy. This prolonged grieving process can sometimes lead to complicated grief or post-traumatic stress disorder (PTSD).
- Stigmatization: In many communities, there’s a persistent stigma associated with suicide. Families of the deceased might face social isolation, with community members either avoiding them out of discomfort or assigning blame.
- Generational Impact: Children who lose a parent or sibling to suicide are at a higher risk for depression, anxiety, and suicidal ideation themselves. The trauma can disrupt their developmental process, leading to academic challenges, behavioral problems, and difficulties in forming relationships.
- Breakdown of Family Structures: The emotional toll can strain relationships within the family. Spouses might drift apart, siblings might experience increased conflict, and the overall family cohesion might be compromised.
ECONOMIC IMPLICATIONS
- Loss of Income: If the deceased was a primary breadwinner, the family could face immediate economic hardships. This is especially acute in rural areas where farmer suicides leave families with debts and reduced means to earn.
- Medical and Funeral Costs: The process leading to the suicide might involve medical expenses, especially if there was a suicide attempt before the actual act. Moreover, funeral costs can be a burden, further straining the family’s finances.
- Nationwide Economic Impact: On a macro level, the premature loss of working-age individuals impacts the nation’s productivity and potential GDP growth. There are also indirect costs involved in terms of medical care, counseling, and other support services.
PSYCHOLOGICAL EFFECTS ON SURVIVORS
- Survivor’s Guilt: Those close to the deceased often grapple with intense feelings of guilt, constantly questioning their actions and wondering if they could have intervened.
- Increased Risk of Mental Health Disorders: Survivors, especially immediate family members, have a heightened risk of developing mental health conditions, including depression, anxiety disorders, and PTSD.
- Suicidal Ideation: Exposure to suicide increases the risk of suicidal ideation in survivors. They might view suicide as a viable option to escape their overwhelming grief and guilt.
- Need for Therapy and Counseling: The trauma can necessitate long-term psychological support. However, due to the stigma associated with both suicide and mental health services, many might avoid seeking help, exacerbating their distress.
CHALLENGES IN ADDRESSING THE ISSUE
INSUFFICIENT DATA COLLECTION AND RESEARCH
- Inadequate Reporting: Not all suicides are reported, and many are often misclassified due to societal pressures, stigma, or administrative oversights. The actual numbers could be much higher than what’s officially recorded.
- Lack of Comprehensive Studies: While the National Crime Records Bureau (NCRB) provides yearly statistics, there’s a dearth of in-depth research studying patterns, causes, and other qualitative aspects of suicides in India.
- Under reporting of Suicide Attempts: Due to legal and societal implications, suicide attempts are often under reported. Without this data, it becomes challenging to understand the extent of the crisis and design effective interventions.
STIGMA AND SOCIETAL NORMS
- Silence Surrounding Mental Health: The cultural and social stigma surrounding mental health issues often prevents individuals from discussing their challenges openly or seeking help.
- Misunderstandings about Suicide: In many communities, suicide is misinterpreted as an act of cowardice, a crime, or a sin, rather than a manifestation of deep psychological distress. Such misconceptions can deter preventive measures.
- Pressure to Conform: Societal norms, especially regarding academic and career achievements, gender roles, and marital expectations, exert significant pressure. Speaking out or seeking help against these norms can be challenging for many.
RESOURCE CONSTRAINTS IN RURAL AND UNDERSERVED AREAS
- Limited Mental Health Professionals: India faces a stark deficit of trained mental health professionals. As per a World Health Organization (WHO) report, there are roughly 0.3 psychiatrists, 0.12 nurses, and 0.07 psychologists per 100,000 people in India. This shortage is even more pronounced in rural areas.
- Inadequate Infrastructure: Many districts, particularly in remote regions, lack dedicated mental health facilities, compelling individuals to travel long distances for treatment.
- Financial Constraints: The cost of mental health care, even if available, might be prohibitive for many, particularly those in the lower socio-economic strata.
- Lack of Awareness: In many rural and underserved communities, there’s a limited understanding of mental health issues. Traditional beliefs, lack of education, and misconceptions can overshadow evidence-based approaches to mental well-being.
PREVENTION AND INTERVENTION
GOVERNMENT INITIATIVES
- Mental Healthcare Act 2017: This landmark legislation not only decriminalized suicide but also emphasized the rights of individuals with mental health issues to seek and receive quality care.
- District Mental Health Programme (DMHP): Launched as part of the National Mental Health Programme (NMHP), DMHP aims to provide mental health services at the grassroots level, especially in rural and underserved areas.
- National Suicide Prevention Strategy 2022: While still in the proposal phase, there have been ongoing discussions about implementing a dedicated nationwide strategy, involving multi-sectoral collaborations and evidence-based interventions.
- KIRAN: The Ministry of Social Justice and Empowerment has launched a 24/7 toll-free helpline “KIRAN” to provide support to people facing anxiety, stress, depression, suicidal thoughts and other mental health concerns.
- Manodarpan Initiative: Manodarpan was an initiative of the Ministry of Education under Atmanirbhar Bharat Abhiyan. It was aimed to provide psychosocial support to students, family members and teachers for their mental health and well-being during the times of Covid-19.
NON-GOVERNMENTAL ORGANIZATIONS (NGOS)
- Vandrevala Foundation: This organization operates a 24/7 helpline providing counseling to individuals in distress.
- Roshni: Based in Hyderabad, Roshni offers tele-counseling services and has been a beacon of hope for many.
- Mann: This NGO focuses on mental health awareness and early interventions among school and college students.
- iCall: Supported by Tata Institute of Social Sciences (TISS), iCall offers email and tele-counseling services to individuals in need.
COMMUNITY INITIATIVES
Grassroot Efforts to Address and Prevent Suicides:
- Farmer Cooperatives: In states like Maharashtra and Telangana, where farmer suicides are prevalent, community-based cooperatives focus on sustainable agriculture, debt relief, and mutual support systems.
- Community Counseling Centers: In various regions, local groups have established centers where community members can seek guidance, counseling, and support.
MENTAL HEALTH AWARENESS
Efforts to Destigmatize Mental Health and Promote Well-being:
- Mental Health Festivals: Events like “The Mind Diaries” or “The Happy Place” aim to foster conversations around mental well-being, using art, music, and dialogues.
- School and College Programs: There’s a growing emphasis on integrating mental health awareness within educational curriculums. Initiatives focus on stress management, emotional well-being, and building resilience.
- Corporate Initiatives: Recognizing the stress of modern work environments, many corporate offices in India are now providing employee assistance programs, mental health days, and wellness workshops.
CASE STUDY
Kota is a place best known for its abundance of coaching centres. It is the third most populous city in Rajasthan, and a large chunk of that population is attributed to aspirants of medical and engineering entrance tests. In such a setting, intense pressure and soul-tearing competition are at its peak throughout the year. Students go through a traumatizing experience that compares to the most gruesome trials a human being can go through.
In the wake of this plight, Horlicks put together a campaign #fearlesskota to assuage some of the emotional strain that the young inhabitants of Kota go through.
It was executed by asking the mothers of the kids studying in Kota to pack their personalized symbols of love in Horlicks bottles. From home-made butter to Banana chips, the mothers of these kids packed them a wide array of items that reconnected them with their roots.
INDIA’S SUICIDE RATE AND PREVENTION EFFORTS VS. OTHER COUNTRIES
SUICIDE RATE
- India: As per the World Health Organization’s data prior to 2022, India accounted for a significant proportion of global suicides, with a rate that fluctuated around 16-17 suicides per 100,000 people. The numbers, however, varied substantially based on factors like gender, age, and region.
- Global Average: The global average, in the same time frame, hovered around 10.5 per 100,000.
- Comparative Figures:
- Russia: Known for one of the highest suicide rates globally, Russia’s rate stood at approximately 26 per 100,000.
- Japan: While Japan has garnered international attention for its high suicide rate, efforts in recent years brought down the rate to around 14 per 100,000.
- USA: The U.S. witnessed an increase over the years, reaching approximately 14 per 100,000.
- Scandinavian Countries: Nations like Sweden and Norway, often lauded for their quality of life, have rates of around 11-12 per 100,000.
PREVENTION EFFORTS
- India:
- The decriminalization of suicide and the emphasis on mental health through the Mental Healthcare Act 2017 are significant steps forward.
- The National Mental Health Programme and District Mental Health Programme aim to decentralize mental health services.
- However, challenges persist in terms of infrastructure, trained professionals, and awareness campaigns.
- Global Comparative Efforts:
-
- Japan: The country instituted a multi-pronged strategy, incorporating governmental initiatives, corporate responsibility, and public awareness campaigns. Their efforts have led to a decline in suicide rates.
- USA: The U.S. has a National Strategy for Suicide Prevention, involving community-based interventions, helplines, and a strong emphasis on mental health research.
- Scandinavian Countries: These nations prioritize mental well-being, with comprehensive mental health policies, accessible care, and robust public awareness initiatives.
- Russia: Despite its high rates, efforts such as restrictions on the sale of alcohol and increased mental health services aim to bring down the numbers.
THE CONCLUSION: While India has made strides in recognizing the gravity of the issue and implementing preventive measures, decriminalising suicide and enacting mental Healthcare Act, there’s still a long way to go when compared to other countries. The nation’s unique socio-cultural dynamics necessitate tailored strategies suited to India.
Mains Practice Questions:
Q.1 What are the various causes that are driving India’s students to suicide? What can we do to prevent it?
Q.2 Prioritising inclusion and support is the key to suicide prevention. Discuss.
Q.3 The rate of suicide among Indian men is 2.5 times of that among women. Discuss the reasons.
Spread the Word